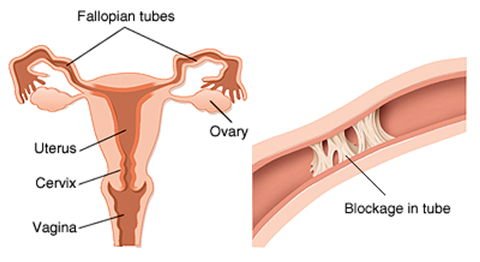
 Fallopian tubes can become blocked without you knowing or feeling it. Women with blocked tubes still ovulate and get their periods. Although sometimes blocked tubes can cause pain, usually you can't feel it at all. Therefore your doctor will need to order a test, if you want to find out whether your tubes are blocked.
Fallopian tubes can become blocked without you knowing or feeling it. Women with blocked tubes still ovulate and get their periods. Although sometimes blocked tubes can cause pain, usually you can't feel it at all. Therefore your doctor will need to order a test, if you want to find out whether your tubes are blocked. 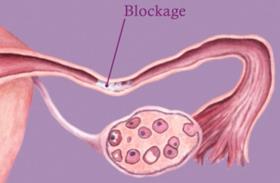
The traditional gold-standard test for determining whether tubes are blocked is called a hysterosalpingogram or HSG. A small tube, or catheter, with a balloon on the end or a stopper-like device is placed into the canal of the cervix. A special liquid called contrast, which shows up white on x-rays, is then infused through the catheter into the uterus and out the fallopian tubes. X-rays are used to watch this happen. It can tell you about the cavity of the uterus as well as whether the tubes are open. It is definitely uncomfortable as the contrast is infused. Usually, it feels like strong menstrual cramps and only lasts a few minutes. Taking some ibuprofen or naproxen sodium beforehand can help, as both of these medications help keep the uterus from cramping. Check with you doctor before taking them, of course. After the HSG, you will have a sticky discharge as that contrast comes back out, so you may want to bring a pad along with you (the ones the x-ray department gives you may be humongous!). The risks to the procedure include infection (rarely, bacteria form the vagina will come along for the ride), allergic reactions to the contrast (tell your doctor about any shellfish, iodine or contrast allergies), and the risk from the small amount of radiation from the x-rays. Sometimes you can get spasms of the tubes that make them look like they are blocked, when the actually are not, too. The test should be done right after your period ends. This way you won't be pregnant when the test is done, and the lining inside the uterus is nice and thin. This helps with being able to visualize the cavity of the uterus well.
Normally, you can't see the fallopian tubes on ultrasound. Mixing something like protein or air, which shows up well on ultrasound, can make the tubes visible, however. Recently, a device called FemVue has made it fairly simple to infuse a mixture of saline with tiny little air bubbles into the uterus and watch it flow out the tubes on ultrasound. This has a few advantages. First of all, there is no radiation like you get with x-rays. Secondly, you can take a look at the walls of the uterus and the ovaries, which you cannot see on an x-ray. It appears to be less uncomfortable too, perhaps because the saline is so much thinner than the contrast used in an HSG. The disadvantage is that you need a doctor who is trained in how to use the device. It has the same risk of infection (rare) as the HSG too.
Finally, the patency of the tubes can be tested at the time of surgery. Saline with a little blue dye can be infused in the same way as it is in the HSG. The surgeon is watching the ends of the fallopian tubes to see if the blue dye comes through.
Some women may not need any of the above tests, though, at least not right away. It has been shown that you can predict most of the women who are going to have blocked tubes by looking at their medical history and doing a blood test for an infection called Chlamydia trachomatis. If a woman has never had any surgery in her pelvis, never had her appendix out, does not have moderate to severe menstrual cramps (signs of endometriosis), and has never had a sexually-transmitted infection or pelvic inflammatory disease (PID); then she is at low risk for tubal blockage. Chlamydia often has no symptoms, and so a blood test should be done to see if she has ever been exposed to Chlamydia trachomatis. If not, then studies show that her risk of having blocked tubes is less than 10%. At that point, both the patient and her doctor can decide whether the doing further testing is worth it.
If your tubes are blocked, then there are several options. If only one tube is blocked, then sometimes just getting you ovulating on the side that is open is all it takes. This will happen about 50% of the time without any intervention, but it is impossible to predict the pattern. Clomiphene citrate (a mild fertility medicine) is often used to get 2 eggs ovulating instead of one. This will increase the chances that at least one of those eggs is on the side that is open.
If both tubes are blocked, then the choice is either to open the tubes or perform IVF (in vitro fertilization or the "test-tube baby" procedure). Because eggs are taken out of the ovaries and then fertilized embryos are placed into the uterus with IVF, the tubes do not need to be open. Unblocking the tubes may or may not be possible. If the tubes are blocked right where they enter the uterus, then it may be possible to open them. Small guidewires can be placed through the blockage to open it up. This can be done under x-ray or with a scope that is placed into the uterus. If the tubes are blocked at the other end, near the ovary, then it also may be possible to open them. This is done by placing a scope and other instruments through small incisions in the bellybutton and down near the pubic bone. The delicate fingers at the ends of the tubes are teased apart. Oftentimes, they are too damaged and scarred together, however, to get apart.
If a woman has had her tubes tied and now wants more children, then the options are also surgery or IVF. The tubes can be sewn back together with very fine suture, if there is enough tube left. The best tubes are ones that were tied at the time of c-section or had a ring or clip put on them. Tubes that were cauterized or "burned" can have severe damage. Many times they cannot be put back together. In that case, IVF is still an option.
No matter how a fallopian tube is opened, doing so puts the patient at risk for a tubal pregnancy. This is when a pregnancy implants in the fallopian tube rather than in the uterus. This can be very dangerous, because there is not nearly enough room inside a fallopian tube for a pregnancy to grow. If not caught in time, the fallopian tube will eventually rupture and the patient will start bleeding into her belly. At this point, it becomes a life-threatening situation. Therefore, women who have had surgery on the tubes or have blocked tubes need to be followed very closely at the beginning of pregnancy. If caught in time, it can be treated with medication.
Sometimes, when the tubes are blocked down near the ovaries, they will fill up with fluid. This is called a hydrosalpinx. The fluid backs up into the uterus and it is very toxic to embryos. If a woman has a hydrosalpinx, then it should be removed. Even if the other tube is open or IVF is planned, removing the hydrosalpinx will keep the toxic fluid from entering the uterus and killing any embryos there.
Fortunately, blocked fallopian tubes make up only a small portion of infertility cases. There is testing that can be done to determine whether a woman's tubes are blocked, for those who are at risk of tubal damage. If one or both fallopian tubes are blocked, there are options.
No comments:
Post a Comment